Differential Diagnosis
For practitioners, the list of potential disorders can include heat stroke, overdose, drug withdrawal, rabies, tetanus, brain abscess, sepsis, encephalitis, malignant catatonia serotonin syndrome, anticholinergic syndrome, lithium toxicity, and meningitis.
The diagnosis of neuroleptic malignant syndrome in a patient includes treatment with neuroleptic drugs within the past 72 hours or the sudden stoppage or reduction of a dopaminergic medication, severe muscle rigidity, fever and altered mental status.
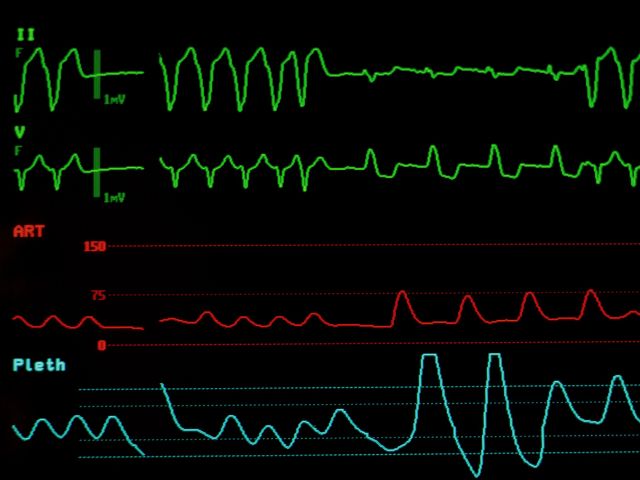
In addition, the patient must have at least two of the following symptoms: diaphoresis, incontinence, trouble swallowing, incontinence, tachycardia, labile blood pressure, leukocytosis, elevated creatine phosphokinase (CPK) and hyporeflexia.